Quick Facts
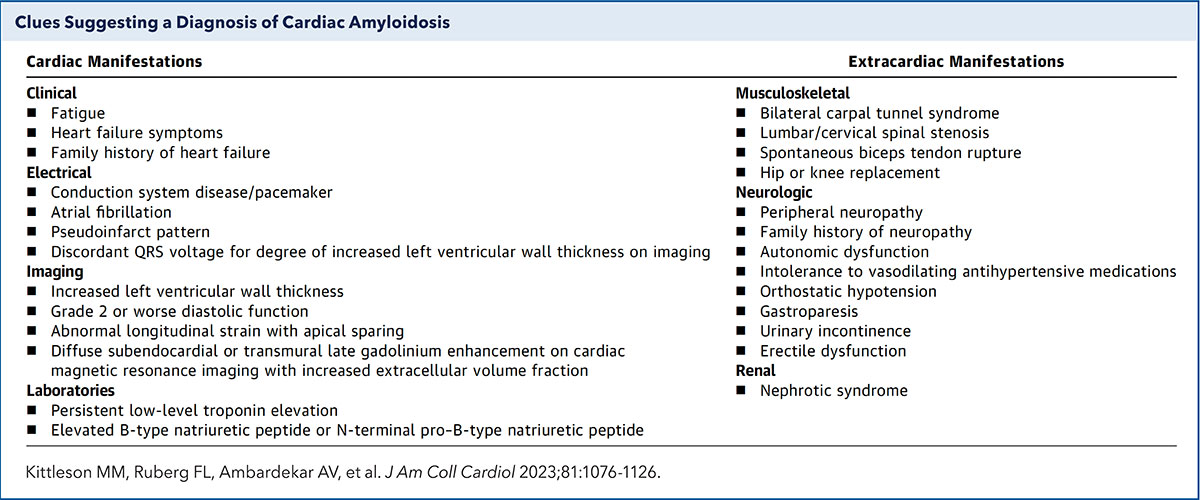
- Critical Alert: Approximately 47% of patients with cardiac amyloidosis receive at least one misdiagnosis before the condition is correctly identified.
- The Carpal Tunnel Link: Bilateral carpal tunnel syndrome appears in roughly 38% of patients and often precedes heart-related symptoms by six or more years.
- Survival Gap: Untreated light-chain (AL) amyloidosis has a median survival of 6 to 12 months, whereas wild-type transthyretin amyloidosis (ATTR) has a median survival of 3.5 to 4.8 years.
- High-Risk Demographics: Elderly men and African American men (particularly those with the p.Val142Ile mutation) are at a significantly higher risk for the ATTR form of the disease.
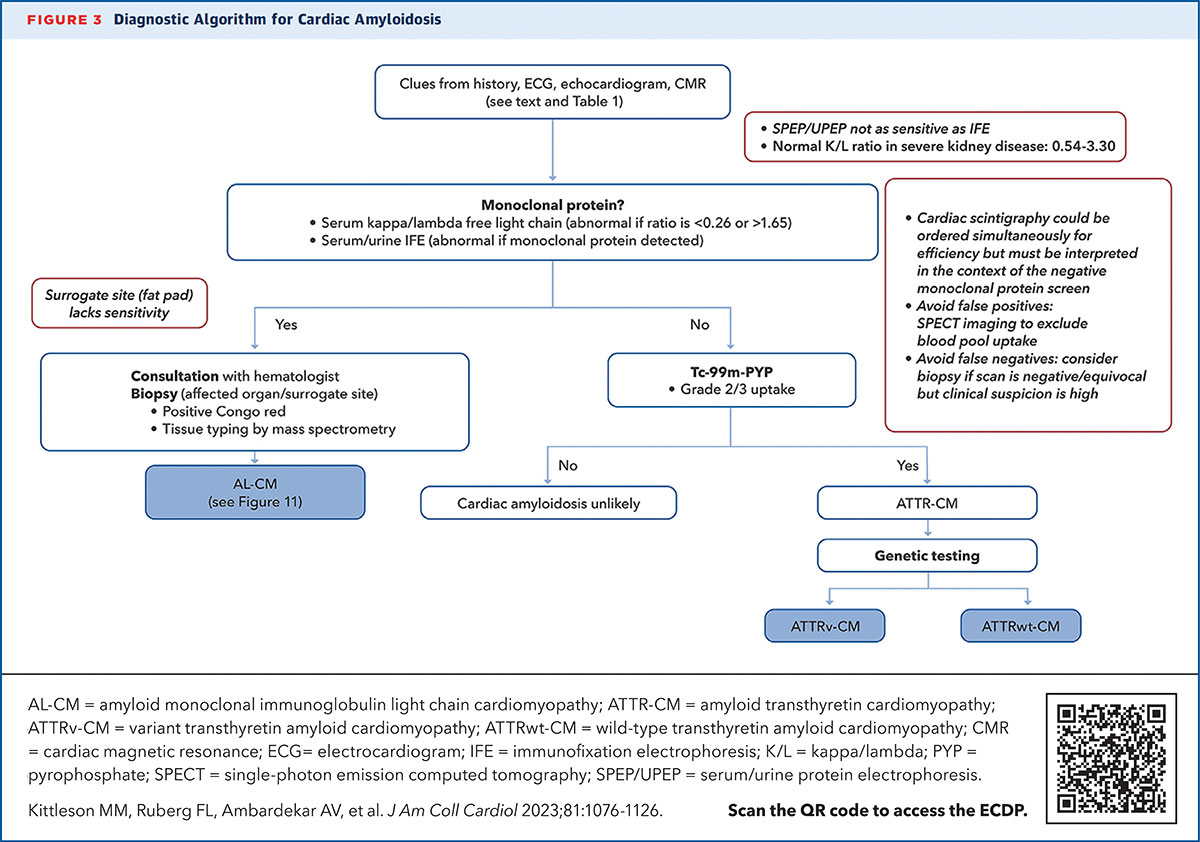
- Diagnostic Shift: Modern medicine has moved toward non-invasive bone scintigraphy and blood screenings, reducing the historical reliance on invasive heart biopsies.
- Early Action: Recognizing non-cardiac triggers like biceps tendon rupture or unexplained weight loss can lead to life-saving preventive care.
Cardiac amyloidosis symptoms primarily manifest as signs of restrictive heart failure, including shortness of breath, lower extremity swelling (edema), and persistent fatigue. These symptoms occur because protein misfolding leads to deposits that stiffen the heart muscle, making it difficult for the organ to fill with blood between beats.
The Orthopedic Prelude: Signs That Precede Heart Issues
For many men, the journey toward a diagnosis does not begin in a cardiologist's office, but in the clinic of an orthopedic surgeon. This is because cardiac amyloidosis is not just a heart disease; it is a systemic disorder caused by the transthyretin protein or monoclonal light chains forming amyloid fibrils. In the transthyretin (ATTR) form of the disease, these fibrils have a strange affinity for connective tissues long before they infiltrate the myocardium.
One of the most reliable subtle early signs of amyloid heart disease to watch for is bilateral carpal tunnel syndrome. While many people associate carpal tunnel with office work or repetitive motion, the amyloid version is different. It often occurs in both wrists and may not respond well to traditional surgery. Research indicates that this condition can serve as a non-cardiac triggers for amyloidosis screening including carpal tunnel history, especially when it presents alongside other orthopedic issues.
Another often-overlooked red flag is a spontaneous rupture of the distal biceps tendon. If you find your biceps muscle suddenly "bunching up" near the shoulder without a significant injury, it could be a sign that protein deposits have weakened the tendon structure. These orthopedic markers represent early signs of amyloid heart disease that provide a critical window for intervention. If you have a history of carpal tunnel in both hands followed by spinal stenosis or unexplained joint pain, your heart may be the next organ involved.
Beyond the Heart: Systemic Red Flags of AL Amyloidosis
While the ATTR form of the disease is often linked to aging or genetics, light chain (AL) amyloidosis is related to a plasma cell dyscrasia. This version of the disease progresses much more rapidly and presents with distinct clinical red flags for cardiac involvement in light chain amyloidosis that are almost unmistakable once you know what to look for.
A primary indicator is macroglossia, or an enlarged tongue. Patients may notice teeth indentations on the sides of the tongue or find it difficult to speak and swallow. Additionally, periorbital purpura—vivid bruising around the eyes, often called raccoon eyes—occurs when amyloid deposits make the small blood vessels fragile. These systemic signs are loud warnings that the body is struggling with a significant protein burden.
Furthermore, amyloid deposits can infiltrate the autonomic nervous system. This leads to autonomic neuropathy, which manifests as orthostatic hypotension and fainting as cardiac amyloidosis warning signs. If you feel lightheaded or dizzy every time you stand up quickly, it may not just be dehydration. This drop in blood pressure, combined with gastrointestinal issues like chronic diarrhea or unexplained weight loss, often forms the early cluster of cardiac amyloidosis symptoms that clinicians miss during routine checkups.
Red Flag Checklist: The "Clinical Detective" Guide
- Bilateral Carpal Tunnel: Numbness or weakness in both hands, often diagnosed years ago.
- Macroglossia: A visibly enlarged tongue or indentations from teeth.
- Periorbital Purpura: Purplish bruising around the eyes without trauma.
- Biceps Rupture: "Popeye" deformity in the arm without a clear injury.
- Orthostatic Hypotension: Significant dizziness or fainting upon standing.
| Feature | AL Amyloidosis (Light Chain) | ATTR Amyloidosis (Transthyretin) |
|---|---|---|
| Primary Cause | Plasma cell disorder (monoclonal light chains) | Transthyretin protein misfolding (Liver) |
| Progression Speed | Rapid; medical emergency | Slow; progressive over years |
| Common Red Flags | Macroglossia, eye bruising, weight loss | Carpal tunnel, spinal stenosis, biceps rupture |
| Typical Patient | Age 50–70; variable | Age 70+ (Wild-type) or younger (Hereditary) |
| Survival (Untreated) | 6–12 months | 3.5–5 years |
The Stiff Heart: Congestive Failure and Structural Signs
As the disease progresses, the heart muscle becomes thick and non-compliant—a condition known as restrictive cardiomyopathy. Unlike typical heart failure where the heart becomes weak and enlarged, cardiac amyloidosis symptoms often appear while the heart’s squeeze (ejection fraction) still looks "normal" on a standard ultrasound. However, because the heart is stiff, it cannot relax to fill with blood, leading to a backup of fluid in the body.
This fluid backup results in identifying right-sided heart failure edema in amyloidosis patients. Look for swelling in the ankles and legs that leaves an indentation when pressed. As the condition worsens, fluid can accumulate in the abdomen, a condition called ascites, leading to bloating and a loss of appetite. You might also notice jugular venous distention, where the veins in the neck appear bulging or pulsating.
It is vital to recognize cardiac amyloidosis symptoms in elderly patients and African American men specifically. In the African American community, approximately 3% to 4% of individuals carry a specific genetic mutation (p.Val142Ile) that significantly increases the risk of hereditary ATTR amyloidosis. For these men, congestive heart failure symptoms in amyloidosis can be misdiagnosed as simple hypertension or "old age," leading to delays in treatment that significantly impact longevity.
Electrical Disruptions and the Modern Diagnostic Workup
The infiltration of amyloid fibrils does not just affect the "plumbing" of the heart; it wreaks havoc on the "wiring." As these proteins move into the heart's electrical pathways, they can cause heart block, atrial fibrillation, or life-threatening arrhythmias. If you experience palpitations or a heart rate that feels consistently too slow, these may be cardiac amyloidosis symptoms reflecting electrical interference.
Diagnosing this "silent intruder" has historically been difficult, contributing to the high misdiagnosis rate where many patients see three or more physicians before getting an answer. However, the diagnostic landscape has changed. We no longer rely solely on invasive biopsies of the heart muscle.
Modern specialists use NT-proBNP biomarkers as a sensitive blood test to detect heart stress. If these levels are disproportionately high compared to the visible damage on an echocardiogram, it triggers further investigation. Advanced imaging techniques like cardiac magnetic resonance (CMR) allow doctors to see the specific pattern of late gadolinium enhancement that characterizes amyloid deposits. Furthermore, bone scintigraphy—a scan traditionally used for bone health—is now the gold standard for identifying ATTR amyloidosis non-invasively, as the tracer binds specifically to the transthyretin deposits in the heart.
Early detection through these methods is the difference between a terminal prognosis and a manageable chronic condition. By the time overt heart failure appears, the damage is often extensive. The goal for longevity is to catch the protein misfolding during the "orthopedic phase" or via early biomarker screening.
FAQ
What are the first signs of cardiac amyloidosis?
The very first signs are often non-cardiac, such as numbness or tingling in the hands (carpal tunnel syndrome) or a sudden rupture of the biceps tendon. In the AL form, an enlarged tongue or unexplained bruising around the eyes may be the earliest indicators before any shortness of breath occurs.
Are there specific red flag symptoms for cardiac amyloidosis?
Yes, specific red flags include bilateral carpal tunnel syndrome, "raccoon eye" bruising, an enlarged tongue, and dizziness upon standing. In the heart specifically, a key red flag is having heart failure symptoms despite a "normal" ejection fraction on an echocardiogram.
Can cardiac amyloidosis cause heart failure?
Absolutely. It causes a specific type called restrictive heart failure. The amyloid proteins make the heart walls thick and stiff, preventing the heart from filling with enough blood, which leads to fluid backup in the lungs, legs, and abdomen.
Why is cardiac amyloidosis often misdiagnosed?
It is often misdiagnosed because its symptoms, such as fatigue and leg swelling, mimic more common conditions like high blood pressure or kidney disease. Additionally, many doctors are not trained to look for the orthopedic "clues" that precede the heart issues by several years.
How do doctors check for cardiac amyloidosis?
Physicians use a combination of blood tests for NT-proBNP and monoclonal proteins, cardiac magnetic resonance imaging (CMR) to look for tissue scarring, and bone scintigraphy (technetium pyrophosphate scan) which can confirm ATTR amyloidosis without a biopsy.
What are the signs that cardiac amyloidosis is getting worse?
Worsening signs include increasing shortness of breath even at rest, significant swelling in the legs and abdomen, frequent fainting spells due to low blood pressure, and the development of irregular heart rhythms like atrial fibrillation.